Serum creatinine is the most commonly measured endogenous filtration marker. It is a 113 dalton amino acid derivative that is generated from the breakdown of creatine in muscle, distributed throughout total body water, and excreted by the kidneys primarily by glomerular filtration. Although the serum level is affected primarily by the level of GFR, it is also affected by other physiological processes, such as tubular secretion, generation and extrarenal excretion of creatinine. Due to variation in these processes amongst individuals and over time within individuals over time, particularly the variation in creatinine generation, the cutoff for normal versus abnormal serum creatinine concentration differs among groups. Because of the wide range of normal for serum creatinine in most clinical laboratories, GFR must decline to approximately half the normal level before the serum creatinine concentration rises above the upper limit of normal. Therefore, the estimated GFR which combines the serum level with other demographic factors that represent these unmeasured physiological variables, provides more information that the serum creatinine alone.
Three commonly used equations are the CKD-EPI creatinine equations, the Modification of Diet in Renal Disease (MDRD) Study equation, and Cockcroft and Gault equation. All three of these equations use serum creatinine in combination with age, sex, weight or race to estimate GFR and, therefore, improve upon several of the limitations with the use of serum creatinine alone.
All creatinine based estimating equations are limited by: (1) use of serum creatinine as a filtration marker; (2) decreased accuracy at higher levels of estimated GFR; and (3) non-steady state conditions for the filtration marker when GFR is changing.
CKD-EPI Equation
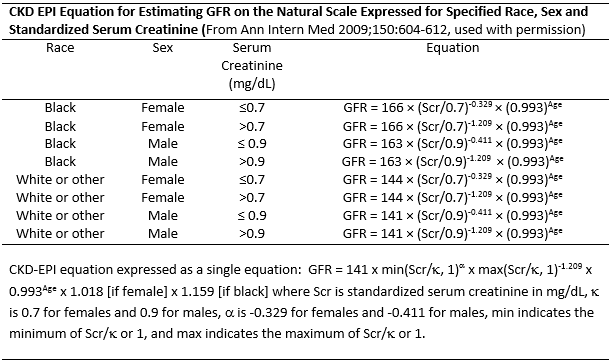
The CKD-EPI equation was developed in 2009 using a diverse population estimate GFR from serum creatinine, age, sex and race. The CKD-EPI equation is as accurate as the MDRD Study equation (currently reported by laboratories) in the subgroup with estimated GFR less than 60 mL/min/1.73 m2 and substantially more accurate in the subgroup with estimated GFR greater than 60 ml/min/1.73 m2. It is the recommended equation in the Kidney Disease: Improving Global Outcomes (KDIGO), Chronic Kidney Disease Guidelines. The table shows the equation expressed as separate equations by level of serum creatinine, sex and race. The footnote at the bottom of the tables shows the equation expressed as a single equation.
MDRD equation
The 4-variable MDRD Study equation was developed in 1999 using data from 1,628 patients with CKD with GFR from approximately 5 to 90 milliliters per minute per 1.73 m2. It estimates GFR adjusted for body surface area and is more accurate than measured creatinine clearance from 24-hour urine collections or estimated by the Cockcroft and Gault formula. The equation is:
![]()
The equation was re-expressed in 2005 for use with a standardized serum creatinine assay, which yields 5 percent lower values for serum creatinine concentration:
![]()
GFR is expressed in mL/min/1.73 m2, SCr is serum creatinine expressed in mg/dL, and age is expressed in years.
The Cockcroft and Gault formula
The Cockcroft and Gault formula (CG) was developed in 1973 using data from 249 men with creatinine clearance (CCr) from approximately 30 to 130 mL/m2. It is not adjusted for body surface area. CCr is expressed in milliliters per minute, age in years, weight in kilograms:
![]()
CG is no longer recommended for use because that it has not been expressed using standardized creatinine values.
Last Updated: July 2014